GENDER AFFRMING SURGERY & RECONSTRUCTIVE UROLOGY
445 East 77th Street
New York, NY 10075
(212) 241-4812

GENDER AFFRMING SURGERY & RECONSTRUCTIVE UROLOGY
445 East 77th Street
New York, NY 10075
(212) 241-4812


Dr. Purohit presenting at the American Urological Association
Rajveer Purohit is the Director of Reconstructive Urology at the Icahn School of Medicine at Mount Sinai Hospital in New York City, and senior faculty in the Department of Urology. Dr. Purohit specializes in complex pelvic reconstructive surgery such as urethral strictures and fistula repair and gender affirmation surgery such as vaginoplasty, metoidioplasty and phalloplasty.
In 2018, Mt. Sinai appointed him co-director of its first fellowship in Reconstructive Urology that trains methods of gender affirmation surgery including vaginoplasty, metoidioplasty and phalloplasty.
Quick Links
Introduction to Genital Gender Affirmation Surgery for Transgender Women
Introduction to Genital Gender Affirmation Surgery for Transgender Men
Introduction to Transgender Care
Phalloplasty Options





See Our Main Site At RajveerPurohitMD.com
Blog Posts Are Below:
In early March, Dr. Purohit was honored to be invited as a renowned international expert to teach a Masterclass on Gender Affirmation Surgery in India to over 120 Plastic Surgeons. He presented 4 lectures focusing on his techniques to optimize cosmetic and functional outcomes.
Gender Affirmation Surgery Topics included:
The talks were very well received and he was asked to light the “Diya” or light of knowledge at the end of the conference.




Dr Rajveer Purohit Clears All Doubts On Coronavirus, Lauds India’s Lockdown Measure
https://www.facebook.com/IndiaToday/videos/was-newyork-not-prepared-for-pandemic-/504016633600850/
https://www.facebook.com/ndtv/videos/covid-19-on-the-availability-of-ventilators/512192282779930/
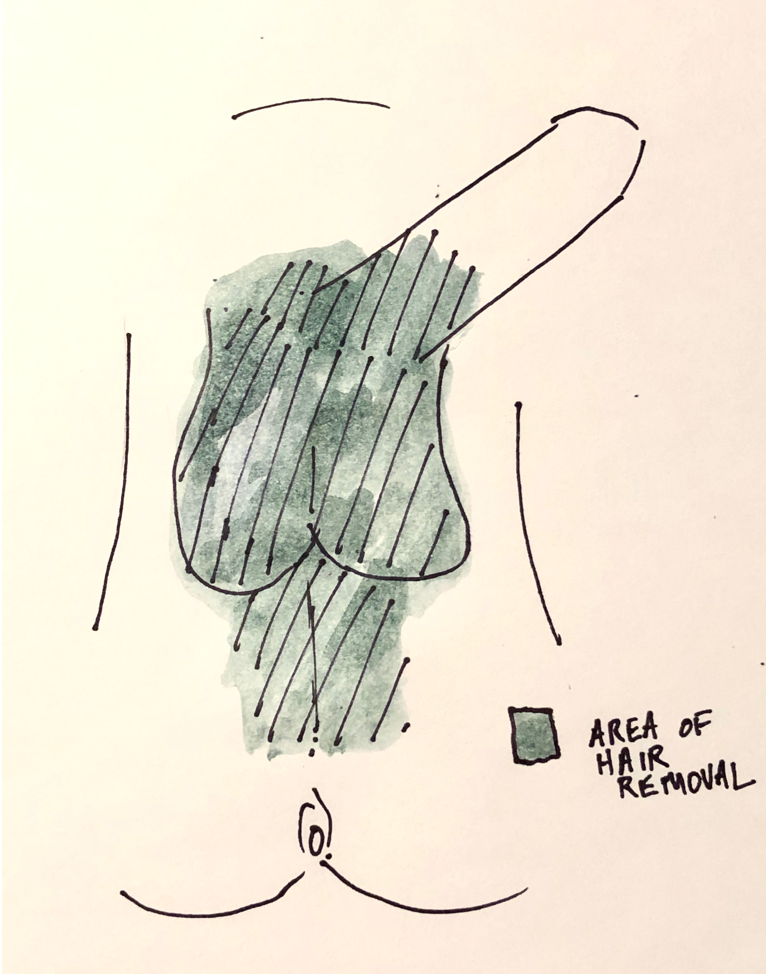
Often with penile inversion vaginoplasty, skin from the scrotal or pelvic area is used to create the new vagina. Some of this area, however, contains hair which can continue to grow even after the skin is used to create the new vagina. In addition to being unsightly, the vaginal hair can create an odor, mucous, even stones inside the vagina. Once it has formed it is difficulty to permanently remove hair once it grows inside the vagina. For this reason, preoperative permanent hair removal is critical for having a good postoperative outcome.
For penile inversion vaginoplasty we use the following template for where the hair should be removed:
 Should I Remove All of the Hair Before my Vaginoplasty? What is the Best Method?
Should I Remove All of the Hair Before my Vaginoplasty? What is the Best Method?Generally, I advise patients to leave some hair above the phallus as this will leaves aesthetically appropriate hair in the mons region above the vagina after penile inversion vaginoplasty. If you don’t want that pubic hair you can always have it easily removed after surgery.
Shaving, tweezing or waxing the hair helps to remove hair in the short run but the hair tends to grow back. There are two methods of permanent hair removal that are commonly used: electrolysis and laser.
Electrolysis uses electrical energy to destroy the root of the hair and, unlike Laser treatments, it has the same effect on patients regardless of skin or hair color. But, with electrolysis only small patches of hair can be removed at once and patients typically require multiple visits for complete hair removal.
Laser hair removal uses a laser to destroy the roots of the hair. Because it targets darker pigment, it is generally best for patients with light skin and coarse, dark hair – the laser can sometimes burn darker colored skin and leave the skin with patchy lighter colored areas. The advantage of laser hair removal is that it permits large areas of hair removal at once and can be quicker to remove large areas of hair prior to surgery. If hair does come back, it tends to come back a little lighter than before.
We are fortunate to have a laser available at Mount Sinai for our patients undergoing gender affirmation surgery. Health insurance generally does not cover hair removal, we have had some success getting coverage for laser hair removal when it is done at Mount Sinai. If your insurance does not cover hair removal, electrolysis is generally cheaper than laser hair removal – although costs can vary greatly.
Hair removal can take time to schedule and I always tell my patients to start the process as soon as possible after their initial visit with me. It is sometimes the step that delays getting your vaginoplasty completed. If you do not live close to New York City hair removal can be done locally to speed up the process.
For more information, call today:
Rajveer Purohit, MD, MPH
445 East 77th Street
New York, NY 10075
(212) 241-4812
Vaginal dilations are a very important part of your recovery process after vaginoplasty. Dilations keep the vagina open preventing vaginal stenosis – a process where the vaginal walls scars down and contract. The new vagina has a tendency to close because the body’s reaction to any procedure is to scar and try to heal itself – although in this situation this “healing” process is counterproductive.
After your vaginoplasty you will be sent home with a new set of vaginal dilators. Bring these dilators with you on your first visit to the office.
When you are discharged home you will have a catheter in place to drain the bladder and a packing left in the vagina. This packing is very important as it allows the vagina skin to heal and “stick” to the underlying tissue. During this time, as you recover, it is important to avoid any vigorous activity in part because you don’t want to have incisions disrupted but also because it allows time for the vaginal grafts to “take” which in the long term increase the chances of a good outcome.
 Soul Source Dilators
Soul Source DilatorsThe dilators you will be sent home with are usually from a company called Soul Source and come in four different sizes and colors (https://www.soulsource.com/collections/grs-vaginal-dilators). The dilators are gently angled at the tip to conform with with angle of the vagina. In addition, their are dots alongside the length of the dilators which correspond to the depth. If you are able to get the dilator to the final dot on the dilator then that is 6 inches of vaginal depth (a pretty good result!).
About one week after surgery when you come into the office he vaginal packing will be removed. This can be a little uncomfortable and the packing itself can have an odor to it. Once removed, I’ll show how to use the dilators by starting on the purple size (the thinnest dilator).
After you get home you should dilate once. Always use lubrication when you dilation. Often patients will start with metronidazole gel which can be used as a lubricant as well. For the first 2 weeks after surgery you should dilated twice a day for about 20-30 minutes each time. After 2 weeks you can increase the frequency of dilation to 3 times a day. After a month you can start to go up on the size oft eh dilatory to blue then green and finally orange. Consider increasing the size of the dilator if the dilator goes in easily to the final dot and you don’t have any discomfort placing it.
If the dilations are getting more difficult or the vagina is feeling tighter when you dilate you should dilate more frequently every day until it is easier to get the dilator in. You can also leave the dilator in for longer periods of time if it is difficult to dilate.
Make sure the dilator is clean before dilation and after dilation you can just wash out the dilator with a mild soup and water. It should be kept clean but does not have to be sterile.
You should also douche with a minimal amount of gentle soap and mostly water to keep the vagina clean starting about 2 weeks after surgery. Women typically will do this in the shower or on the toilet. Periodic douching washes out remnants of the lubrication and can hep decrease bacterial overgrowth.
Vaginal dilations are important to minimize one of the more common risks after vaginoplasty – vaginal stenosis or closure of the vaginal canal. But do different techniques of penile inversion vaginoplasty have different risks of vaginal stenosis? Unfortunately, like so many things in the field, there isn’t great comparative data on this topic. At a very basic level there are 2 types of tissues that we typically use to create the vaginal lining: tissue flaps or tissue grafts. The difference between the two is that flaps are still connected to their own blood supply while grafts are not- grafts survive initially by sucking up oxygen from surrounding tissue until new blood vessels develop over the course of a few days. Because of this blood supply difference, grafts have a higher chance for contraction and vaginal stenosis. The penile skin in the penile inversion vaginoplasty is a flap and scrotal or peritoneal skin are grafts.
So how do you minimize the risk of vaginal stenosis? Use as much of a flap as you can to create the vaginal lining. So this mean using as much penile skin as possible. Sometimes, patients have enough tissue to create a deep 6 inch vagina but in many cases there isn’t enough tissue to do this. In this case, before surgery you should decide whats important for you – If you want to absolutely minimize risk of stenosis and penetrative vaginal sex or vaginal depth is not important to you then you might stick with the penile flap and not add additional depth with a graft. if depth is important and there is not much phallic skin then you would almost certainly want additional depth with a graft and accept the risk of stenosis and post-op be very diligent about dilations.
Although there are disadvantages to using colon for a vaginoplasty, one of the advantages is that the segment of colon has its own blood supply so that the risk of stenosis is very low.